Acne is a chronic inflammatory disease of the pilosebaceous unit. Acne commonly occurs in adolescence and in
young adulthood. Typically, significant acne will spontaneously regress in early adulthood; however, a number of
people will experience persistent acne or new-onset acne in adulthood.
The American Academy of Dermatology (AAD) defines acne
as a “chronic inflammatory dermatosis notable for open or
closed comedones (blackheads and whiteheads) and
inflammatory lesions, including papules, pustules, or
nodules.” Papules typically present as variably
erythematous lesions of less than 5 mm. Pustules are
discrete white fluid-filled papules of 5 mm or less. Larger
lesions (5 mm or more), also with variable erythema, are
termed “nodules.” The deeper structures, such as pustules,
nodules, and cysts, can form tunnels or sinus tracts and
often result in severe scarring especially when they form
close to one another.
Although the exact cause of acne is not fully established, it is generally accepted that multiple factors are involved.
Presently, research points toward four main processes that contribute to the development of acne. Keys to the
pathogenesis of acne are Propionibacterium acnes (P. acnes), keratinocyte hyperproliferation in the follicle,
androgen-mediated increase in sebum production, and, most importantly, inflammation. These factors cause the
cutaneous microenvironment to change and leads to inflammatory reactions of the host that foster acne lesion
progression.
Propionibacterium Acnes
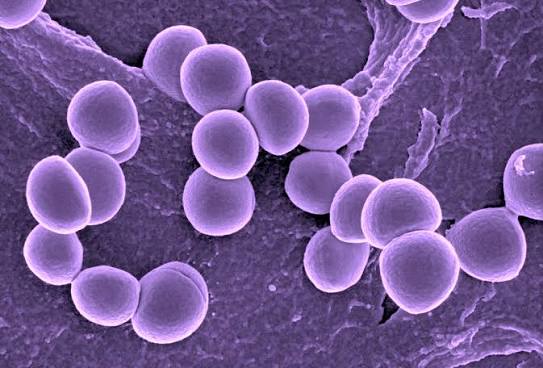
P. acnes is one in a group of normal gram-positive bacterial flora found in the follicular unit. The exact contribution
to the skin made by this bacterium is not clear. Some studies show increased bacterial load in those with clinically
evident acne, but this is not universally confirmed.There is a significant increase in P. acnes colonization at puberty,
the time during which acne commonly develops, and teenagers with acne can have as many as 100-fold more P.
acnes bacteria present on their skin than healthy, age-matched counterparts.
It is believed that the bacterium can stimulate tumor necrosis factor-alpha and the interleukins. Specifically, IL-1β,
IL-8, and IL-12 seem to be stimulated by P. acnes.
1 A 2016 study showed that when P. acnes is trapped in an
airless environment such as alongside hair and skin cells, it turns the sebum into fatty acids that active inflammation
in nearby skin cells.2 Usually, this inflammation is switched off by histone deacetylases, but the fatty acids deactivate
these enzymes so that the inflammation can continue unchecked.
In healthy skin, P. acnes plays a role in the protective immune response by contributing to the formation of shortchain fatty acids and in maintaining a more acidic skin pH. A lower skin pH promotes keratinocyte growth and is
less hospitable for bacterial growth. In healthy skin, as opposed to acne skin, structural differences have been seen
along with variances in immune modulation carried out by various P. acnes strains.
Gram-Negative Folliculitis
Gram-negative folliculitis is an infection caused by gram-negative organisms. This type of infection can occur as a
complication in patients with acne vulgaris and typically develop in patients who have received systemic antibiotics
for prolonged periods.4 In acne patients treated with oral antibiotics, the number of gram-positive bacteria decreases
but the number of gram-negative bacteria such as enterobacterial organisms increases by more than double.4 The
bacteria populate existing acne lesions and cause superficial pustules with relatively few papules and comedones.
Because the cell wall structure of gram-negative bacterium contains a thin peptidoglycan layer, traditional treatments
with antibiotics which target peptidoglycan synthesis are not as effective. This makes gram-negative folliculitis
difficult to treat with common western medicine prescriptions or creams.
Androgen-Mediated Increase in Sebum Production
Sebaceous glands secrete oil or sebum. Sebum works to protect the skin against friction, reduces moisture
penetration through the outer skin layers, and acts as part of the healing process.1 Disrupted follicular keratinization,
a component of pore blockage, can occur with changes in sebum. Changes in sebum—production, increase,
composition, and oxidant-to-antioxidant ratios—are all seen with acne formation.1 If these changes in
sebum interferes with the process of follicular keratinization in the pilosebaceous unit, pore blockage may occur,
contributing to lesion formation and acne.
Increased sebum production is stimulated by an increased androgen activity in the pilosebaceous unit. The
increased androgen activity is related to an excess in androgen hormones or an increase in sebaceous gland
sensitivity to normal androgen levels or increased activity of 5α-dihydrotestosterone (5α-DHT) in the skin. 5α-DHT
is considered the major proponent of increased sebaceous gland activity as the glands contain the necessary
enzymes involved in the conversion of testosterone to 5α-DHT. An increase in testosterone causes an increase in
sebum production because testosterone is one of the major androgens that interact with the androgen receptors
on sebaceous glands.
In females, menstruation can cause an increase in sebum production due to changes in hormone levels. Just before
menstruation, estrogen and progesterone levels decrease. This triggers the sebaceous glands to secrete more
sebum. When the female hormones drop, testosterone stays level throughout the whole month. This also triggers
sebaceous gland activity and the resulting clogged pores when testosterone levels are higher than both the female
hormones. These fluctuations in hormones can also trigger skin inflammation which can increase the production of
acne-causing bacteria.
In both males and females, liver health can play an important role in chronic acne. Since the liver is involved in the
regulation of hormones, a liver deficiency can also lead to an increase in sebum production. The liver metabolizes
estrogen which increases sex hormone-binding globulin (SHGB). SHGB binds to free testosterone in the blood
stream to inhibit testosterones effects. If the liver is not metabolizing estrogen at the proper rate, there can be an
increase in the free testosterone in the blood which contributes to the acne development.
Viral Infections
Poxvirus is a type of virus that results in the formation of lesions, skin nodules, or rashes. Infection in humans usually
occurs due to contact with contaminated animals, people, or materials. While some poxviruses, such as smallpox
(variola virus), no longer exist in nature, other poxviruses can still cause disease. These include monkeypox virus, orf
virus, molluscum contagiosum, and others.
Molluscum contagiosum is an infection caused by a poxvirus that results in mild skin disease characterized by lesions
that may appear anywhere on the body. Within 6-12 months,
Molluscum contagiosum typically resolves without scarring but may take as long as 4 years. The lesions, known as Mollusca, are small, raised, and usually white, pink, or flesh-colored with a dimple or pit in the center. They often have a pearly appearance. They’re usually smooth and firm. In most
people, the lesions range from about the size of a pinhead to as large as a pencil eraser (2 to 5 millimeters in diameter). They may become itchy, sore, red, and/or swollen. Mollusca may occur anywhere on the body including the face, neck, arms, legs, abdomen, and genital area, alone or in groups.
Although not limited to children, it is most common in ages 1-10 years of age. Children and adults are most at risk
who suffer from a weakened immune system, those with atopic dermatitis, and those who live in a warm and humid
climate. Atopic dermatitis can increase the risk of getting Molluscum contagiosum due to frequent breaks in the skin.