Condition of the Month-
-
" class="aMenuButton-page text-center">Download the Entire Protocol of the Condition
Login as practitioner to view Wellness Recommendation.
Fibromyalgia syndrome (FMS) is a condition characterized by widespread pain, and “tender points” of the muscles and joints on the neck, shoulders, back, hips, arms, and legs. The pain can occur systemically or migrate throughout the body and typically comes and goes over time. FMS is most common in women but can also occur in men and usually arises in middle adulthood. FMS can be hard to diagnose since there are no tests or diagnostics to determine if an individual has FMS. However, practitioners can suspect fibromyalgia in patients with mostly musculoskeletal pain that is not due to injury or inflammation.
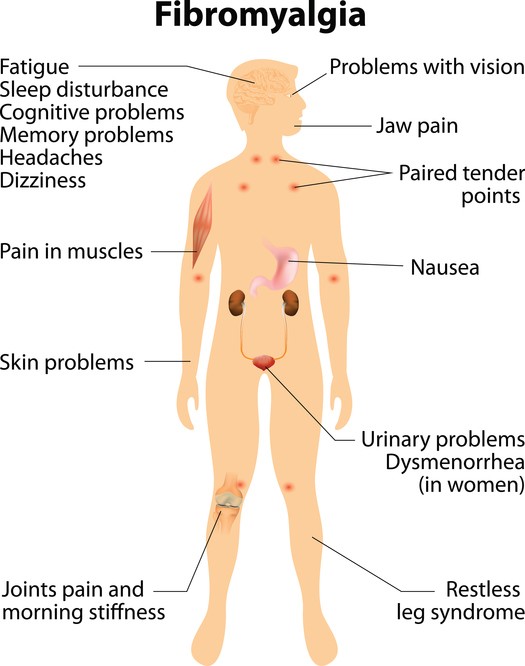
Besides widespread pain and tenderness of the muscles and joints, symptoms of FMS also include fatigue, sleep problems, headaches, anxiety, depression, poor memory and problems with thinking or cognitive difficulties. These cognitive difficulties are commonly referred to as “fibro fog” which impairs the ability to focus, pay attention, and concentrate on mental tasks. FMS can co-exist with other conditions such as irritable bowel syndrome, migraines, interstitial cystitis, or TMJ.
FMS can be either primary, also known as idiopathic fibromyalgia, or secondary. In primary fibromyalgia, the cause is unknown, or the trigger is no longer in existence. However, primary fibromyalgia can be related to a past acute stress such as an acute bacterial or viral infections or from a reaction to certain drugs. Whereas in secondary fibromyalgia the cause is clear and is tied to a physical injury or a chronic infectious disease that coexists with the fibromyalgia condition. Such physical injury can include a neck injury, stenosis, herniated or bulging discs, ankylosing spondylitis, or trauma that is particularly in the upper spinal region. The chronic infectious diseases include Lyme disease, Hepatitis C, HIV or endometriosis. Primary fibromyalgia is the more common form.
Physical or mental stress from a disease or trauma can trigger microcirculation re-distribution and cause ischemic muscle pain. The peripheral microcirculation reduction due to vasoconstriction triggered by stress acts via the sympathetic nervous system which activates the hypothalamic-pituitary-adrenal (HPA) axis. The HPA axis is the central stress response system. Stress results in cardiovascular dysfunction with vasoconstriction which causes reduced peripheral blood flow in primary fibromyalgia, although the transient stress is gone, the peripheral vasoconstriction is still persistent. In secondary fibromyalgia, the stress and the resulting vasoconstriction are chronic. Overtime, this reduced blood flow leads to the development of ischemic muscle pain.
Microcirculation redistribution not only affects the muscles but also the central nervous system in FMS patients. Previous studies have shown a decreased amount of blood flow to the parts of the brain that provide an emotional response to pain and an increased amount of blood flow to the part of the brain that processes pain. This can alter neuron metabolism and brain activation. The neuromatrix which is activated in response to painful stimuli has been seen to be more pronounced in these patients. This can cause a highly amplified pain sensation to a pain signal as well as cause symptoms of anxiety and depression. Reduced cerebral blood flow is also observed in fibromyalgia patients. This can cause brain fogginess and affect cognitive function.
In addition to widespread muscle pain from the vasocontraction, FMS patients also present with cutaneous hyperalgesia, an increased intensity of pain sensation of the skin. Nociceptive input from deep tissues sensitizes the spinal neurons resulting in the abnormal pain sensation from the skin. This is why FMS has been described as a Central Pain Amplification disorder meaning the volume of pain sensation in the brain is turned up too high.
Nitric Oxide (NO) alteration and oxidative stress is also seen in FMS patients. NO participates in many physiological processes such as vasodilation, modulation of nociception, neurotransmission, and excitation-contraction coupling. Stress induced microcirculation re-distribution can cause decreased levels of NO which further reinforce the microcirculatory disturbances. This may explain the persistence of vasocontraction after the initial stress factor has gone away in primary fibromyalgia patients. Oxidative stress due to decreased blood flow can also affect RBCs since they are susceptible to free radical damage. A study done at Stanford found that chronic fatigue patients have RBC that are no longer round and take longer to enter the capillaries and flow through them. This may keep them from delivering the correct amount of oxygen to the cells which further aggravate the oxidative stress and cause chronic fatigue symptom in FMS patient.
A decreased supply of oxygen to the muscles and cerebrum in FMS can affect the amount of ATP produced by the cells mitochondria which can cause tissue acidosis in these areas. High levels of oxidative stress constrict the blood vessels making nutrient delivery deficient. Insufficient amounts of ATP production and other nutrient deficiency in muscles and cerebrum causes not only chronic fatigue but also brain fogginess, sleep issues, headaches, anxiety, depression, poor memory and decreased cognitive function such as math difficulties.
Chronic pain patients also have a higher rate of ingesting pain killers at an attempt for symptom relief. Long-term use of pain killers can cause liver damage and liver toxicity. The liver is innervated by and is involved in the processes of the autonomic nervous system. When the liver is weakened it can cause an abnormal neurological repair mechanism which can also result in an abnormal pain response. This may be an additional factor in fibromyalgia pain.
" class="aMenuButton-page text-center">Download the Entire Protocol of the Condition